
All things recycle; history, fashion, design, even topics of conversation. Assimilating endometriosis to cancer is the latest recycling topic among our community.I agree with our community regarding the injustices endometriosis and those with the disease endure. Poor understanding and awareness over many decades has created a situation on par with a poorly sealed pressure-cooker. Frustration and anger continues to build within our community; temperatures rising in response to poor awareness, knowledge and interventions for the disease.
Validation of the disease, allocation of resources and acknowledgement of the sufferer’s experience is long overdue. In addition, the degree of burden on families, peers and employers is rarely appreciated. Despite the glacier-like rate of progress to understand pathogenesis of endometriosis, enough rudimentary knowledge about endometriosis has led to comparatives of endometriosis and cancer. True, numerous similarities exist between endometriosis and cancer, but should we be comparing them? The naked truth: to feel like, or want to die, versus the uncertainty that you may, or know you will die, can’t be compared.
Despite similarities between cancer and endometriosis, there are also differences. I’m not here to judge or condemn anyone who equates endometriosis to cancer. However, I hope to expose each reader to physiological, societal, historical and cultural aspects that have, and continue to influence how we perceive endometriosis. From my personal perspective, comparisons transpired from society’s ignorance about endometriosis and sufferers attempt to communicate it’s potential destruction.
Thankfully I’ve not faced a diagnosis of cancer. If I did, I imagine my first thoughts might be:

A diagnosis of endometriosis can be devastating. It does not directly threaten the life of a person, but for some, it threatens the ability to bring another life into the world. It can ruin intimate relations, impact ability to complete education, hold a job or career, hobbies, self/family care or household chores. Each in their own way, those with either disease often worry about passing along their disease genetically.
Inherited?
Undisputed evidence exists, inheritance plays a role in development of cancers and endometriosis. Our environment (nutrition, chemical exposure, stressors etc) also influence activity of genes and DNA mutations that lead to disease.
Genetic changes that cause cancer can be inherited from our parents. They can also arise during a person’s lifetime as a result of errors that occur as cells divide or because of damage to DNA caused by certain environmental exposures. (1)
The heritability of endometriosis has been estimated at around 50% based on large twin studies. (2)
It has been demonstrated that first-degree relatives of women with this disease are more likely to develop endometriosis. And when there is a hereditary link, the disease tends to be worse in the next generation. (3)
One disease?
Cancer is known to be a collection of multiple diseases. “There are more than 100 types of cancer”.(1) In contrast, endometriosis is considered a single disease. However, at present, there is international collaboration among institutes and clinics across the globe to determine if endometriosis is really a ‘single disease’ or comprised of multiple subtypes.(4)
Tumors and lesions:
Most cancers form solid tumors; those of the blood, such as leukemia, generally do not. Cancers may be Benign (debateable) or Malignant. Benign disease is encapsulated. It is not the cell properties that separate benign from malignant disease; it is the presence of a capsule barrier which restricts cancer cells form infiltrating surrounding tissues. Hence, the inability to infiltrate local tissue or break off and travel to another part of the body restricts benign tumours to a single, location. Hence, most ‘benign’ tumours are confined to a single site with low probability of regrowth after removal.
“… benign tumors do not spread into, or invade, nearby tissues. Benign tumors can sometimes be quite large, however. When removed, they usually don’t grow back, whereas malignant tumors sometimes do. Unlike most benign tumors elsewhere in the body, benign brain tumors can be life threatening.(1)
Malignant disease is not contained by a capsule. There are no barriers to restrict growth and spread of the cancer cells. Cells can rapidly reproduce, invade surrounding tissues and can ‘break off’. With exception to blood and lymphatic types, malignant cancers originate from a single site. When cells from the primary source dislodge, they can travel to other locations in the body. This satelite lesion(s) are metastasis(es). Like the primary site, these metastases also grow, unregulated..The type of malignant cancer cells a metastatic tumor ‘breaks off’ from determines the tissue(s) and organ(s) of the body it invades.
“Cancerous tumors are malignant, which means they can spread into, or invade, nearby tissues. In addition, as these tumors grow, some cancer cells can break off and travel to distant places in the body through the blood or the lymph system and form new tumors far from the original tumor.” (1)
Similar to cancer (malignant), some forms of location invade the surrounding tissues (deep infiltrating endometriosis), other forms remain superficial, located in a thin layer that covers the surface of the body cavities (peritoneum). While the origin(s) of endometriosis is yet to be proven, unlike cancer, the distribution of endometriosis throughout the body as satellite cells from a single, primary endometriosis lesion.(1) It is probable, based upon evidence, that some locations of endometriosis arise from (ie lymphatic and vascular) distribution. However, in addition to the uterus, stems cells from the bone marrow are two potential remote sources of endometriosis cells. But, these are not metastases, given that neither are malignant. Last, it must be acknowledged that local specialized cells may transform into endometriosis lesions directly at the site.(5) In this scenario, each endometriosis lesion would be considered a primary lesion.
The National Cancer Institute describes cancer into categories of Benign (debatable) and Malignant based upon cell containment. It is the presence of a barrier between cancer cells and body tissues that prevents unregulated growth, potential to spread to other areas of the body and invade tissues. Scientists who focus on cell properties and behaviours; investigate disease at the cellular level, hold the position that all cancers are malignant. In other words, their are ‘benign tumours’, not ‘benign cancer’. Cancer properties include ability to infiltrate other tissues and spread. These are properties of cancer.
“Tumours can either be benign or malignant, Cancer is the name given to a malignant tumour”……..”The word cancer only applies to malignant tumours. There is no such thing as a benign cancer. So, by definition, all cancers are malignant tumours.” (6)
The basics of cancer and endo:
Unlike benign tumours, endometriosis is rarely a single lesion. They are similar, in that, if the entire lesion is removed, probability of regrowth in the same location is very low. Endometriosis, benign tumours and malignant cancer can all be silent or symptomatic.
Similar to malignant cancers, endometriosis lesions can invade local tissue.
Malignant cancers are divided into those which form solid masses or affect the vascular and lymphatic systems. Endometriosis consists of disease divided into three divisions: ovarian, superficial peritoneal and deep infiltrating endometriosis (DIE).
Expanding the prior topic about the classification(s) of endometriosis, an ongoing project by the World Endometriosis Research Foundation’s (WERF) goal is to establish subtypes of the disease (based on characteristics of lesions), acquire evidence suggestive of one or more origins of the disease, and develop individualized treatments based upon disease subtypes. In addition, subtyping endometriosis lesions may reveal relations of endometriosis and specific types of cancer (not just gynecological) beyond an ‘association as co-morbid diseases’. To clarify our present knowledge:
“Before endometriosis can be linked with evidence to any type of cancer, more methodologically-robust research will need to be undertaken.” (3)
With exception of vascular and lymphatic disease, cancers develop from a primary site. Secondary sites result from a primary tumor ‘breaking off’, travelling to another location in the body (metastases). Primary and secondary sites of malignant cancers are genetically identical. Although some theories speculate endometriosis occurs from distribution of cells from a single primary site (the uterus) by way of retrograde menstruation, evidence of initial attachment and the genetic composition of endometrial cells of the uterus (eutopic) and those of endometriosis lesions (ectopic) are genetically different. Further, we know genetic variation occurs among endometriosis lesions within the same person. Both characteristics contrast malignant, metastatic cancer.
Cancer cells are less specialized than normal cells. That is, whereas normal cells mature into very distinct cell types with specific functions, cancer cells do not. (1)
The risk of a benign tumor’s conversion to malignancy is dependent upon the type of tissue(s) the benign tumor developed from.(1) The risk of endometriosis (specifically ovarian) conversion to cancer is estimated at 1.8%.(3)
Sex hormones, cancer and endo:
Some forms of malignant cancers (ie. breast, uterus, prostate, testicular) and endometriosis are sensitive to androgens (sex hormones). Exposure to sensitive specific androgens promote growth of specific types of cancer and endometriosis.
Director or influencer of self-growth?
Cancer and endometriosis manipulate their environment to meet their needs. However, each disease does so differently.
In regards to cancer, its cells ‘ignore’ the body’s attempts to control the lesion’s cellular division. This leads to rapid growth of the cancer. Cancer also influences, ‘orders’, surrounding tissues to grow blood vessels, bringing nutrients and oxygen, further promoting its growth.(1)
Endometriosis cells don’t ‘ignore’ the body’s orders to stop, like cancer cells. Instead, endometriosis lesions produce products that reduce the number of ‘clean up cells’, ‘rubbish/trash collectors’ in the immune system. As a result, the slowed rate of cell death and clean up allows a net growth of endometriosis lesions. Unlike cancers, endometriosis lesions create vascular and neural tissues through their own cellular processes. This differs from cancer cells which direct other tissues to create these structures.
Mortality and morbidity rates:
Cancer impacts children, men and women proportionally.
Cancer is among the leading causes of death worldwide. In 2012, there were 14.1 million new cases and 8.2 million cancer-related deaths worldwide. Approximately 38.4% of men and women will be diagnosed with cancer at some point during their lifetimes (based on 2013–2015 data).(1)
Endometriosis primarily impacts cis-females, often becoming symptomatic around menarche and can continue post-menarche. It’s estimated to affect 1:10 women around the world. A small portion of cis-gender males and transgender persons develop endometriosis but the disease is predominantly limited to cis-females. The probability a woman will be diagnosed with endometriosis is 10%. Among those with endometriosis, risk of lesion conversion to cancer is 1.8%. In contrasts, the probability for any cancer diagnosis during a cis-female’s lifespan is 38%.
What about the Pain?
Unless you’ve had both, is it appropriate to make comparative statements when you’ve not directly experienced both? It’s acknowledged that the degree of pain, symptom profile and other unpleasant experiences among both diseases are wide ranging. Some malignant cancers are silent. Some endometriosis is silent. It’s also widely acknowledged that non-invasive medical management for cancer is often more debilitating than the disease itself. In contrast, there is little awareness and acknowledgement among the general population, of severe side effects that can occur with non-invasive medical management for endometriosis. However the endometriosis community is painstakingly aware (detailed below with additional links including links).
The type of pain varies with the form of cancer and treatment. Similarly, not all endo pain is the same. Both disease symptom profiles are associated to the organs and tissues involved. Similar systemic issues can arise with both diseases to include fatigue and anaemia. Further, both diseases may lead to the removal of body organs or cause organ dysfunction and/or death.
Is there a cure?
Cure rate for cancer is dependent upon the type of cancer and it’s staging (stage 1-4). Some malignancies have no cure. The physiological advancement of cancer directly reduces the lifespan of many persons.
There is no cure for endometriosis. However, it’s important to reiterate, endometriosis does not directly shorten the life of a person through growth of the disease. (It’s vital to acknowledge a handful of special scenarios death from the disease has and can occur. A few cases include 3 deaths from bilateral renal death and 1 death due to a large lesion inside the heart. All (4) cases occurred prior to development of soft tissue imaging equipment. A true definition of ‘cure’ is not established for the disease. Ongoing critically ill cases with resolution are periodically reported in the scientific literature primarily with disease within the respiratory and urinary/excretory systems).
Treatments, often as bad, or worse than the disease:
(For sake of blog length, this section is limited to a simple overview).
Treatment for cancer may include radiation, chemotherapy and surgery. Traditional treatment for endometriosis includes medical management and/or surgery. Most people have a cursory understanding of cancer treatment, either through personal experience or that of a loved one. Treatment for cancer and endometriosis have some common side effects to include fatigue, memory loss, altered bone density, joint pain and hair loss.
Hormone Suppressants
However, outside of the endometriosis community, most members of the public, and even those within the healthcare sector, are oblivious to consequences of some medical therapies still used today. A variety of hormone manipulating medications are used reduce the symptoms of endometriosis. Some forms (ie oral contraceptive pills/birth control – tier 1) are tolerated well by most individuals. Other, (tier 2) have higher probability of side effects list of long-term side effects is longer.
One classification in-particular physicians prefer in their treatment plan are GnRH agonists and GnRH antagonists. (GnRH-a). GnRH-a Our specific attention here is to Lupron (GnRH- agonist) and the newer, ‘replacement’, Orilissa. The links below are recent investigative news reports (video and written), primarily about Lupron:
(Investigative report – video clip)
KTNV Channel 13 Las Vegas: More women come forward about complaints of Lupron side effects
(investigative report – video clip)
San Diego women speak out about highly controversial drug injection
(video clip – investigative report)
Georgia woman says drug used to treat endometriosis led to series of health problems
(written investigative report – hormone suppressant off-label use to delay puberty)
Women fear drug therapy they used to halt puberty led to health problems
A 2014 interview with Lynne Millican, RN (founder of Lupron Victims Hub.). Includes multiple testimonies of persons whose treatment included the use of Lupron.
Lupron: a nightmare produced by Abbvie
It’s important to recognize that the patent for Lupron recently expired. The drug is now available at a lower cost in generic form. Lupron is replaced with a new patented hormone suppressant, Orillisa. Through a slightly different mechanism, it also lowers estrogen production by the ovaries. Note: Orilissa was released for public access 2018. The extent of all side effects, short and long term are yet to be known. Only recently, the media has taken interest in the adverse effects of Lupron, for some women they continue decades after exposure to the medication. Will this same scenario occur with those exposed to Orilissa?
An independent, non-profit panel of healthcare practitioners, provides and insurance providers participated in analysis of reports from Orilissa drug trials prior to it’s FDA approval. Findings of the report can be reviewed at:
Institute Clinical Economic Review Final Report for Elagolix (Orilissa)
(Note: page 77: Comparative Clinical Effectiveness Figure 3.1 ICER Evidence Rating Matrix; page 78: Table 3.12: ICER Ratings on the Comparative Health Benefits of Elagolix; 158-160 personal testimonials)
Surgery:
Ablation may address superficial endometriosis lesions (to a depth of 1-2 mm) but does not remove deeper disease. Ablation also leaves charred debri and eschar, properties known to activate the immune system, enhancing the inflammatory response. This leads into the topic of disease ‘recurrence’ vs ‘remaining unaddressed disease’. Its an important concern that should be considered when ‘new disease’ when there has been a prior surgical intervention. Further, scientific publications comparisons of ablation vs excision – report variable outcomes, but poor control for surgeon skill and experience. Excision of lesions (cutting out) the disease has lower ‘recurrence rate’ than ablation, among experienced surgeons with advanced training in the technique. At present, excision is the closest intervention to’ a cure’.
The requisite skills to surgically remove endometriosis, which often impacts the organs among multiple body systems overlap those used among oncology surgeons.
Historical perception and impact on today’s perception of disease:
For decades, the majority of health studies limited study participation and analysis to men. At the time, it was universally believed that the inability to control for the natural, biological process of menstruation and cycling of hormone levels in women would diminish data accuracy. For decades, data collected exclusively from males was erroneously applied to women. The scientific community has only recently (about the last decade or so) improved inclusion of women among studies of diseases that impact men and women.
Unfortunately, attention (to include funding) dedicated to Women’s Health specific remains severely neglected. Limited quantity of completed studies, data collected and allocated resources to conduct them remains a barrier to faster improvements in knowledge and treatment of women’s health conditions. Specific to endometriosis, a chronic lack of government funds toward research led to investments among pharmaceutical companies. This influenced the direction of research and emphasis of medical management approaches to treat endometriosis. These issues continue today.
The woman’s position and role in society: contribution to inequality of research, care and perception of women’s health concerns:
Inequality of women with respect to men is a global issue. With exception to a few nations, inequality of women is significant in every aspect: economic, social, health and cultural. A small portion of transgender persons and cis-males are also affected by endometriosis. The transgender community is also marginalized, similar to cis-women. Cancer also affects women. As clarified earlier, there is greater proportionality of those affected by cancers among the genders and life span. It is with sadness that greater than 1/3 (33%) of women will be diagnosed with cancer during their lifetime comparable to 1/10 (10%) with endometriosis.
Funding to investigate cancers has an expansive budget that dwarfs allocated resources for endometriosis. Cancer should receive greater funding than benign diseases. However, lets take a look at funding for a few other benign conditions and the 2017 mortality rate for each. Mortality rates are one factor used to establish the amount of funding a disease is allocated. The graph below represents distribution of funds through the National Institute of Health between 2017 and 2020. Comparatives for Endometriosis, Temporalmandibular Joint disease (TMJ), Interstitial Cystitis, Scleroderma and Uterine Cancer. All diseases are benign with exception to Uterine Cancer (7):

Other contributors to our perceptions of endometriosis:
- lack of accurate information about the disease taught in medical school.
- lack of accurate information distributed among authorative and influential organizations (ACOG, teaching hospitals, etc.) See Blog #2: Another Awareness Month Comes to an End.
- lack of research funding independent of the pharmaceutical industry (above table).
- lack of patient advocate inclusion among policy and guideline discussions (the USA lags behind the United Kingdom, Australia and a few other countries).
- long term barriers of perpetuated myths and misinformation that continue to circulate in medical curriculum, stagnation to update didactic resources, professional continuing education coursework, traditional perception of a gynecological disease has kept pediatricians, general practitioners and other specialists from developing greater awareness and recognition of the disease, contributing to delayed and oft misdiagnosis.
- association of pelvic pain as a manifestation of mental and/or emotional difficulties. The ‘Wandering Uterus’.
Stigma associated with disease and its negative impact:
Stigma associated with Women’s Health still remains. Particularly those associated with menstruation. Although the current Menstrual Movement has improved public acceptance of the topic for conversation, culture and familial beliefs still impart a sense of shame among many menstruators . This makes it difficult-to-impossible for them to distinguish what is normal and abnormal. In addition, endometriosis has historically been perceived as a female reproductive system disease. A gynecological problem. In reality. This has led to silence, confinement behind closed doors or redirection from healthcare providers to the gynecologist to address concerns. In addition, adolescents may not approach their pediatrician about their concerns, which further delays acknowledgement of disease until the adult years.
Further complicating the issue is the poor awareness and recognition that endometriosis can impacts tissues, organs and systems outside of the female reproductive tract. Knowing this, it is vital these areas are included and integrated in the analogies and descriptions we use to convey what it is to have endometriosis.
Public response to ‘I have cancer’ is far different to ‘I have endometriosis’ or, ‘I have pain down there’. Of course we know many would respond with comments such as ‘Never heard of it’ or, ‘I get bad cramps (with my period) too’. Even, ‘My mom/friend/other had that. They just got a hysterectomy’. It’s sad that the conversation around endometriosis has remained virtually unchanged for decades. Sufferers of the disease still face belittling comments, that depreciate the real sufferers experience.
Where do we go from here? How do we convey the destructive nature of endometriosis without using cancer as a comparative?
We could build on a few established analogies many can relate to or conceptualize. A few of these, often reiterated by an endometriosis advocate leader, Nancy Petersen, RN (ret) include: The pain of endometriosis is –
“… ‘on par’ to acute appendicitis”
..“on par to or worse than labour pains of birthing”
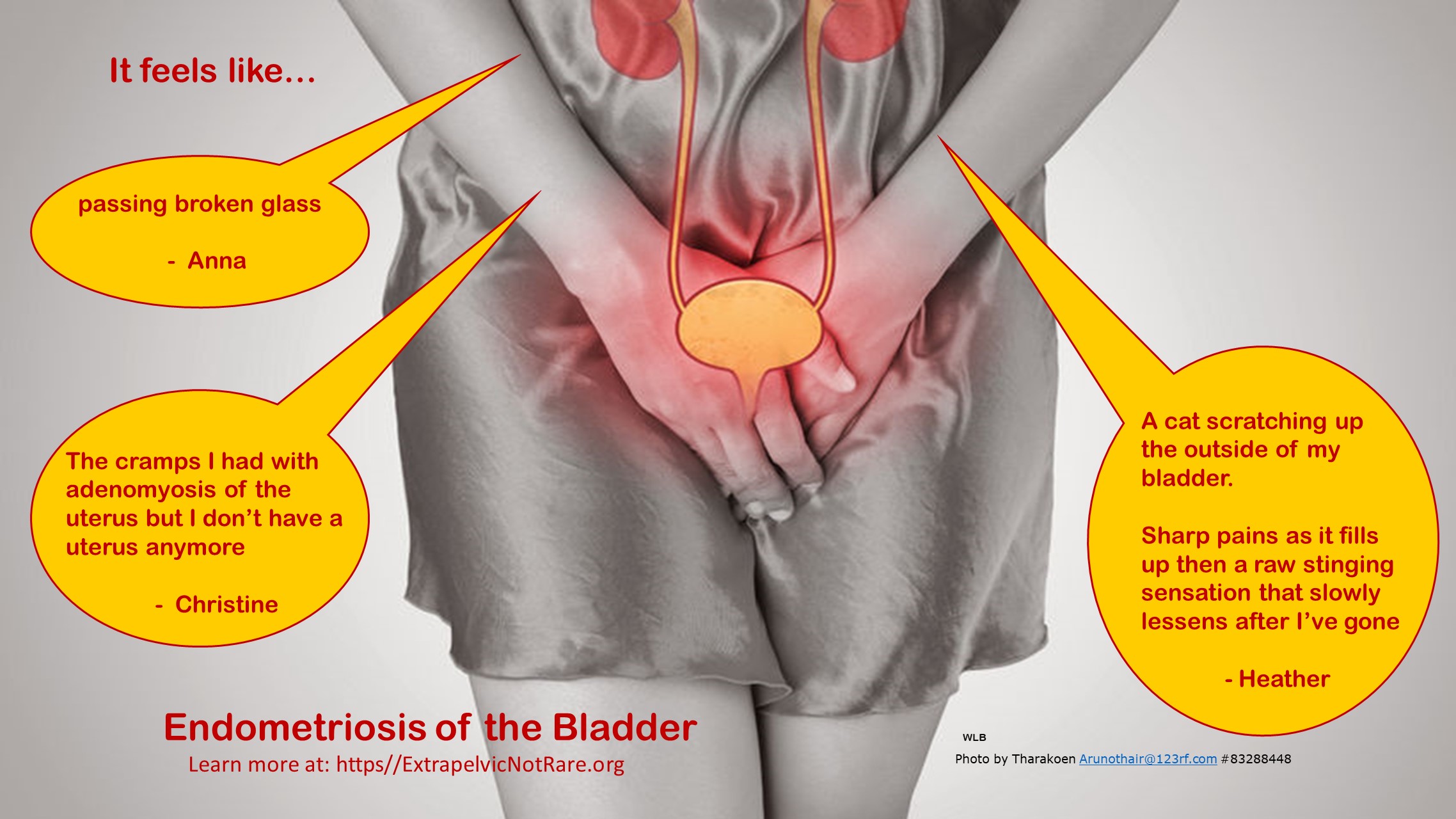
Members of our FB Support Group: Extrapelvic Not Rare, have provided a few analogies of their experience of endometriosis among a few extrapelvic organs:
Bladder:

Intestines:


Chest Cavity and Diaphragm:
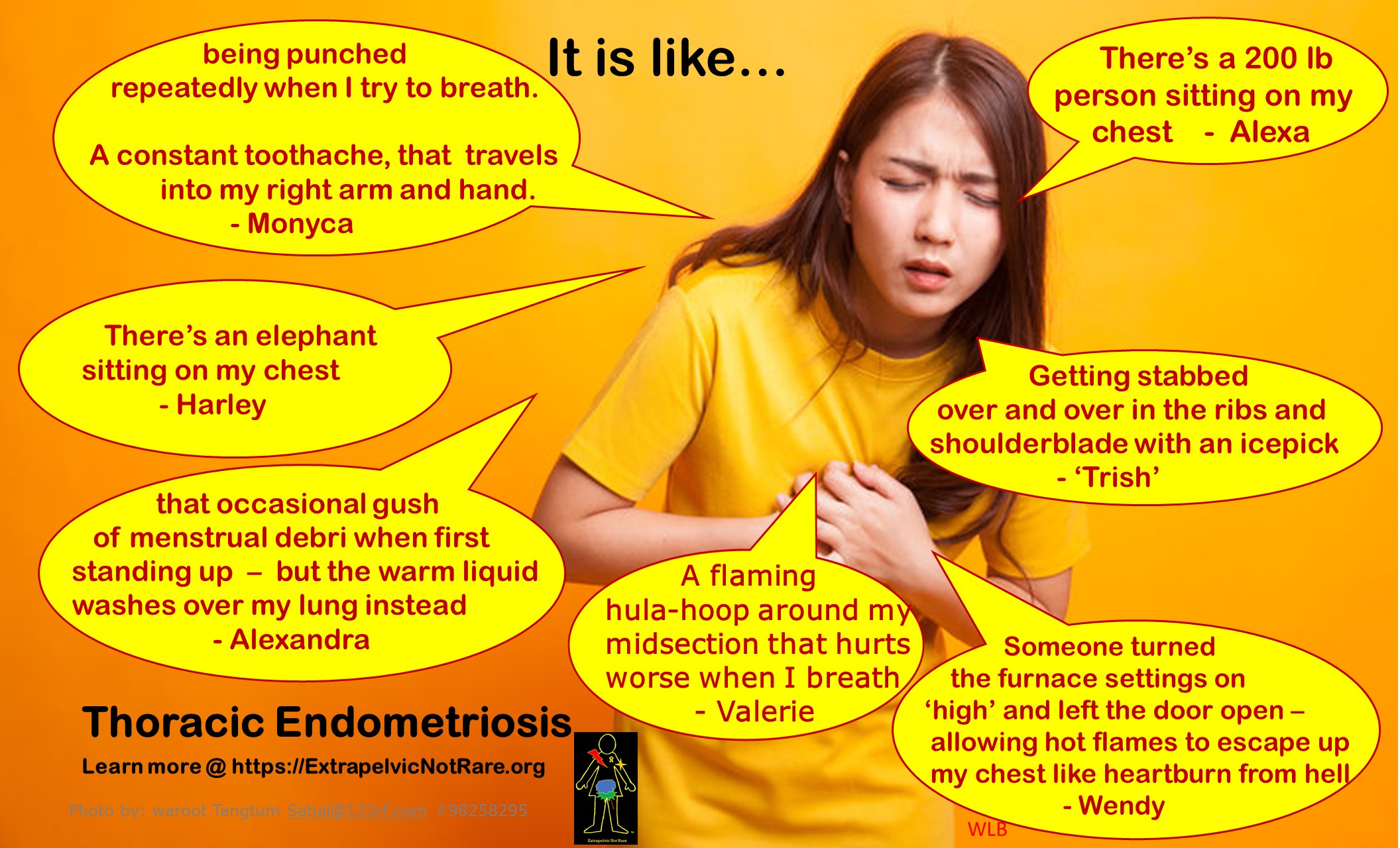

Endometriosis is a benign disease, without direct threat to a persons’ lifespan. But, it should not be dismissed by the medical system and public for this. The review of its similarities to cancer reveal the disease to be far more complex than a simple ‘menstrual complaint’ and ‘inconvenience’. Endometriosis, like a few other benign diseases can be very destructive in all aspects of the person’s life AND negatively impact those around them. If we continue sharing personal testimonies, exchanging knowledge and establishing powerful analogies others can directly relate to or conceptualize, comparison to cancer wont be necessary.
Summary:
You may decide this blog’s reinforced your perception that endometriosis is ‘alike’ to cancer and justifies comparison. OR It may have heightened your perception that endometriosis deserves greater respect and validation. We can develop a conversation that articulates the potential depth of physical destruction, loss of productivity, and quality of life endometriosis can steal without comparison to cancer.
As awareness, education and voices of personal experience create familiarity among all peoples’, the need or desire for comparison to cancer will diminish. Eventually, the adversities and hardship those with endometriosis face, will be conveyed in a ‘stand alone’ statement. I have cancer. I have diabetes.
Just what do we hope to convey exactly? Despite the average person’s lack of familiarity with intricacies of these diseases (cancer, diabetes), instant empathy and a sense of each disease’s potential destruction is understood. There is no need to compare cancer or diabetes to another disease.
I have endometriosis
In reality, injustices toward endometriosis, those with the disease and women’s health have been present for centuries. They remain today. However, when we compare endometriosis to cancer, our attempt to validate the severity and nature of our disease, invalidates cancer in the process, minimizing reality cancer can take a human life, endo does not, directly.
Trish, January 27th, 2020 Tweet Trish’s Blog
References:
1.) National Cancer Institute. http://www.cancer.gov (accessed January 10th, 2020)
2.) Recent Insights on the Genetic and Epigenetic on Endometriosis. Clinical Genetics.
2016. B. Borghese et al. https://doi.org/10.1016/j.fertnstert.2018.10.013
3.) Causes. Endometriosis.org. Hummulshoj L et al. (accessed January 17th, 2020)
4.) World Endometriosis Research Foundation. Endometriosisfoundation.org/ephect
(accessed January 17th, 2020)
5.) Stem Cells and Pathogenesis. IE Sasson, HS Taylor (accessed March 18th, 2020)
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC3107843/
6.) Basics of Oncology. Das, Prasanta. (accessed January 27th, 2020)
https://www.academia.edu/26402833/Basics of Oncology
7.) Estimates of Funding for Various Research, Condition, and Disease Categories
(RCDC). National Institute of Health (published April 19, 2019)
(accessed Jan 17, 2020) https://report.nih.gov/categorical_spending.aspx