
Appendix: Where is it, what’s it look like, what’s it do?
 The Veriform Appendix extends from the large intestine close to the junction of the small intestine. The Iliocecal valve separates the small and large intestines. The Iliocecal valve prevents contents of the large intestine from travel back into the small intestine.
The Veriform Appendix extends from the large intestine close to the junction of the small intestine. The Iliocecal valve separates the small and large intestines. The Iliocecal valve prevents contents of the large intestine from travel back into the small intestine.
 The Veriform Appendix extends from the Cecum. The first section of the large intestine. The Veriform Appendix is a small tube extending from the Cecum.
The Veriform Appendix extends from the Cecum. The first section of the large intestine. The Veriform Appendix is a small tube extending from the Cecum.
The Veriform Appendix (referred to as ‘Appendix’) can be short as 5cm, long as 35 cm. It’s average length is 9 cm.(1)
Sometimes the appendix is located behind the cecum or ileum; in front of the ileum and can extend into the inguinal area (crease of hip). Positioned here, the appendix can create a Amyand Hernia.(1)

Some people are born without an appendix, some can have two or three of them! Its not common but, the size of other pelvic organs can cause the appendix to be found up under the liver – in the right upper quadrant (its normally located in the right lower quadrant).
It was believed the appendix was a remnant of our ancestors; no longer a purposeful organ. Recently, it appears the appendix has a purpose. It contributes to the health and maintenance of our intestinal tract. Its location is ideal to ‘store’ additional bacteria that contribute to our gut health and assist production of neurotransmitters. Episodes of diarrhea remove ‘good’ bacteria that normally inhabit our intestines. The appendix, replenishes the large intestine with ‘good bacteria’.(2)
The walls of the appendix are identical to the intestinal tract. The walls are composed of five layers (1):
-
-
-
-
-
- Serosa
- Muscularis Externa
- Submucosa
- Muscularis Mucosa
- Lamina Propria
-
-
-
-
Appendectomy is the most common surgery performed around the world.(1) However, there are many other causes for abdominal pain of the right lower abdomen that are important to consider dependent up the persons cis-gender and medical history.
_____________________________________________
Differential Diagnosis
Right Lower Quadrant Pain
In addition to Acute Appendicitis, RLQ pain also occurs with other conditions:
Ectopic Pregnancy Pelvic Inflammatory Disease (PID Diverticulum of Cecum Irritable Bowel Syndrome (IBS) Ileocecal Tuberculosis (TB) Amoebic Typhlitis
Classical presentation of acute appendicitis:(1)
Periumbilical pain that migrates to the R LQ (McBurney’s Point) Anorexia (loss of appetite) Body Chills Fever Diarrhea Nausea Vomitting Rebound Tenderness Suprapubic Pain Leukocytosis (↑white blood cells-WBC’s)
Common causes of Acute Appendicitis:
Patient medical history, clinical examination and tests (labs, imaging etc) establish a working diagnosis for Acute Appendicitis. The cause may not be determined until observation at surgery or histological testing after appendectomy.
Diverticulosis Endometriosis Enterobius Vermicularis Granulomatous Cyst Inflammation Mesenteric Cyst Mucoceles Polyps Protozoan Infections Polyps Tuberculosis Tumors * * Tumors include: Adenocarcinoma, Carcinoid, Cystadenoma, Ganglioneuromas, Paragangliomas, Lymphoma, Mucinous Cystadenoma (1,4,5,6,7)
“Endometriosis ranks eight among conditions mimicking appendicitis” (8)
– Kinoo SM (2016)
Imaging to identify ‘acute appendicitis’ and endometriosis of the intestinal tract:
Imaging that details soft tissue structures also detect inflammation associated with appendix, peritonitis and endometriosis. Imaging includes Ultrasound (US), Computed Tomography (CT) and Magnetic Resonance Imaging (MRI).(1) It’s important know that each type of imaging has an inherent limit to detect pathologies. In addition, factors such as (individual anatomy and movement impact clarity of image and interpreters experience.
“Magnetic Resonance Imaging (MRI) is currently the best imaging modality for enteric endometriosis with a sensitivity of 77%-93%. Endoscopy (use of a scope inserted into the intestinal tract ie. colonoscopy) may provide non valuable results because of the intact mucosa (endometriosis lesions infrequently penetrate all the intestinal walls to the lumen), but it is still recommended in all patients with suspected endometriosis to rule out mucosal involvement and malignant lesions with the help of biopsies if needed.”(6) – Ehsani N et al (2012)
Blood samples are helpful to detect anemia and infection. No blood tests are able to detect presence of endometriosis.
Treatment
Most appendices are like a dead-end street: debris enters and exists one-way. It’s a perfect design to trap debris and promote infection. Endometriosis lesions can narrow or completely block the lumen, Lesions can also impede blood flow to areas of the appendix. AE may prompt muscular contractions within the walls and prompt cell death by restriction of blood flow. If infection develops, expansion of the appendix with festering infection and cellular death within the walls from ischemia, risk of rupture rises.
Rupture of an appendix leads to dispersal of infection and debris in the abdominal-pelvic cavity. A dangerous, and potentially life-threatening condition called peritonitis, can occur.
To minimize these risks, acute appendicitis is treated with surgical removal of the appendix. In specific cases, it may be appropriate to initiate an antibiotic regimen, monitor the individual and defer surgical removal for a short period of time.
_______________________________________________
Endometriosis of the Appendix (AE)
History:
-
- The first case of AE was recorded by Von Rokitansky in 1860.(9)
- The first large scale study of AE (135 cases) analyzed publications from 1860 to 1951.(10)
- The first observation AE could ‘mimic’ acute appendicitis was recorded in 1952; a case misdiagnosed as Acute Appendicitis prior to surgery. (11)
- Observation that AE may cause symptoms outside of the menstrual period were made by the end of the 1950’s.(12)
Prevalence:
- AE among all persons with endometriosis is 1%.(4)
- AE among persons with endometriosis of the gastrointestinal tract is about 3%.(4)
- Persons with Deep Infiltrating Endometriosis (DIE) have a 6x increase risk for AE compared to those with peritoneal disease only. (13)
Our database search revealed scant publications of large numbers of women who underwent surgery for acute appendicitis that recorded causing factors and frequencies. A comparative between three populations of women who underwent surgery and the frequency of AE among each group (Table A). The findings of Table A can’t be applied to larger communities (ie across a city, country or global) but it does provide data for further discussion:
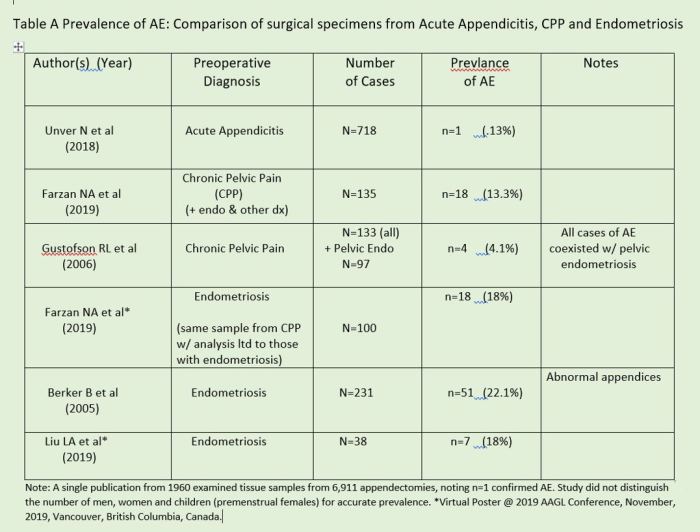
Citations Table A Appendix
In Table A, the frequency of confirmed AE differs in each of the three groups. Frequencies, from highest to lowest among the groups is:
Women with: Pelvic Endometriosis > Chronic Pelvic Pain > Acute Appendicitis
The frequency of AE may be associated to the reason the person underwent surgery. Only a small portion of those with AE develop Acute Appendicitis or a ‘mimicry condition.
Despite being the most common abdominal surgery around the globe, no head-to-head large scale comparison of women undergoing appendectomy vs women undergoing elective surgery for chronic pelvic pain or exploratory surgery for suspicious lesion can be analyzed with good control.
Despite the limitations with Table A, its fitting to ask:
- Is the disease, endometriosis changing? If it is, why?
- Are the numbers a reflection of more surgeries performed across the globe as population rises, accessibility to surgeons with available technology increases (all at different Is technology better to view and analyze samples?
- Are surgeons looking for it more, even when its not their ‘body part’ to address?
- Should surgeons limit appendectomy to those which appear abnormal or should normal looking appendices also be removed?
Reflect on these questions and the next, directly below, when reviewing Tables 1-3.
- Should the current number of slides produced from tissue samples used for histological analysis be increased to diagnose of pathologies of the appendix? Results of a recent study reported a significant increase in diagnosis of AE among 300 women who underwent concurrent appendectomy during pelvic surgery when additional tissue samples were created into additional slides of each appendix.(14)
Profile of persons with AE
-
- AE is identified in persons who are adolescents(1) to post-menopause.(13,15-17)
- The oldest reported case of AE (in our database search) was 77 years old.(18)
- AE occurs in women before and after hysterectomy (with/without ovary removal).(13)
“When the small bowel is affected (with endometriosis), it is generally asymptomatic. If symptoms are present, then they are the result of a chronic obstruction in a majority of cases caused by strictures and adhesions.” (18) – Torralba-Moron A et al (2016)
In response to discovery of active endometriosis in a 77 yo woman presenting to ER: constipation, vomiting, abdominal pain and fever. No history of endometriosis. Preoperative diagnosis based upon CT imaging: tumor of small bowel with perforation (ileum) and intrauterine abscess. Intraoperative diagnosis: intrauterine abscess and fistula connection to the ilium and cecum secondary to intestinal endometriosis. The uterine abscess is postulated to develop as result of intestinal endometriosis development of a communication (fistula) between the ilium and cecum eventually expanding to the uterus.
“Once the disease is established, its persistence and development requires stimulation by estrogens. In case 3, who was not receiving hormone treatment or had any source of endogenous estrogen production, the source of estrogen production may have been the endometriosis focus due to the local production of estradiol, with autocrine and paracrine effects, allowing the progression of the disease or the peripheral conversion of androgens into estrogens in the adipose tissue.” (18) – Torralba-Moron A et al (2016)
-
- A single case of Acute Appendicitis due to AE early into a woman’s third trimester of gestation was identified in our database search.(19)
“The incidence of symptomatic appendiceal endometriosis …. might be (due to) increased hyper-progesteronic states, as it is in pregnancy. “
“Appendiceal endometriosis during gestation (pregnancy) may result in increased incidence of appendectomies for wrongly diagnosed appendicitis.” (19)
– Giorgakis E. et al (2012)
Isolated endometriosis of the appendix
-
- AE can occur in alone (without other endometriosis in the body).(13,20,21)
- AE without presence of endometriosis elsewhere is: Primary AE (3,13,20,21)
- AE present with concurrent pelvic endometriosis is: Secondary AE.(20,21)
“Appendiceal endometriosis is divided into Primary and Secondary forms…The primary form includes histopathological evidence of endometriosis within the appendix with no clinicopathological evidence of extra-appendicular endometriosis. The secondary form is associated with internal and/or external endometriosis.” (21) – Emre A. et al (2012)
Locations of AE
-
- AE can occur on the Tip, Body and Base.(3)
- The majority of AE is evenly distributed at the Tip and Body.(3,22)
- A small portion of AE occurs at the Base.(3,17,19)
Intrinsic and Extrinsic AE
Endometriosis of the appendix is classified like disease of the ureter.
-
- Disease limited to the outer layer: Extrinsic. (Serosa)
- Deeper disease (into or beyond the muscular layers): Intrinsic.
The walls of the appendix are identical layers as the intestinal tract.
-
- About 1/3 of (AE) is Extrinsic.(22)
- About 2/3 of AE is Intrinsic.(22)
Acute Appendicitis is more common with Intrinsic (AE). (11,15)
Intrinsic AE create acute symptoms by blocking the lumen, alter blood flow and lead to infection. It can also create acute symptoms without blocking the lumen. Penetration of endometriosis into or through the muscular layer of the wall can elicit contractions of the appendage. (11,18, 20-25)
The majority of AE is Intrinsic but is involved in a small portion of Acute Appendicitis. Acute appendicitis is also not limited to Intrinsic AE, Infrequently Extrinsic AE can mimic acute appendicitis.
AE is far more common among Chronic Pelvic Pain (CPP) and Chronic Appendicitis (15,26,27) and may or may not contribute to symptoms.
Complications from AE
-
- Bowel Obstruction (partial or complete) (18)
- Bowel/Appendix Perforation (18,19,20)
- Hemorrhage
- Intussuseption (Inversion) (6,16,17)
“Endometriosis involvement of the appendix is usually accompanied by chronic fibrosis, inflammation and hyperplasia or hypertrophy of the muscularis propria” (9)
– Laskou S et al. (2011)
____________________________________
Appendiceal Endometriosis (AE)
grouped by presentation
To date, no ‘text-book’ presentation of AE exists. Observations from 1960 are still relevant today. No single presentation of exists for all AE; but observations over the past century and a half has led to (4) types of presentation. (22)
“There is no clinical syndrome pathognomonic of endometriosis of the appendix. ” (12) – Lane RE (1960)
(1) Acute Appendicitis-like (3,11,18,20,23,25,28,)
(2) Invaginated Appendix (ie intussusception) (6,16,17,28,27)
(3) Non-specific symptoms: colicky abdominal pain, nausea, vomiting, malena (7,9-11,28)
(4) Asymptomatic (prevalence unknown, unclear if + disease contribute to symptoms of CPP in women with endo who undergo excision surgery with appendectomy) (5,12,28)
“Women can present with symptoms mimicking acute appendicitis or chronic pelvic pain” (22) – Lee JH (2013)
___________________________

Citations Table 1 Appendix
- Acute presentation may or may not occur at time of menses.
- Acute appendicitis, or ‘mimic’ acute appendicitis is more common with endometriosis of the appendix penetrates into, or beyond the muscular layer of the wall. However, Acute presentation can also occur among those with endometriosis limited to the outer wall layer.
- Blockage of the lumen may or may not be present with an acute presentation.
- EA occurs with and without the presence endometriosis in the pelvis.
- Our database search: most ‘acute’ case reports did not have history of chronic pelvic pain.
- A small number of ‘acute’ cases reported a history of CPP that progressed to acute.
Mechanisms creating acute appendicitis with AE
“With regards to the pathophysiology of acute appendicitis in the context of appendiceal endometriosis and carcinoid tumour, the data is limited. It seems that there is a degree of luminal obstruction, which increases the appendiceal luminal pressure distally; vascular supply is compromised and this initiates the acute inflammatory response see in cases of appendicitis.” (29) – Kingston, G Farouk R. (2013)
__________________________
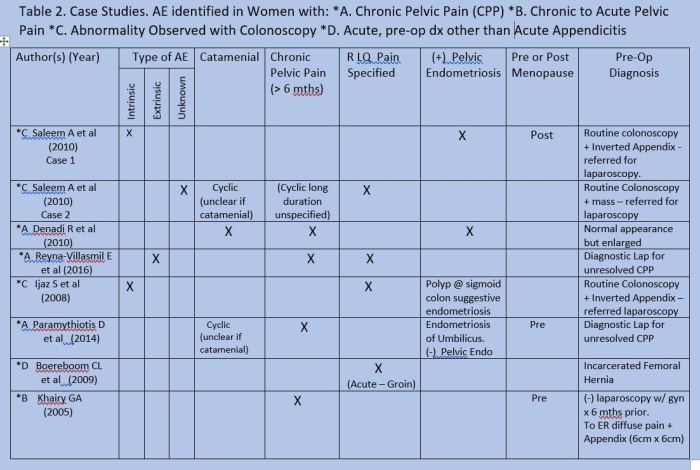
Citations Table 2 Case Studies AE Identified in Women with….
- Some studies report association of Right Lower Quadrant abdominal pain with AE; others found no significant relation. A few cases in Table 2 were identified after referral due to abnormalities detected during routine preventive care examinations (colonoscopy). This occurred among in women with and without a history of cyclic CPP and pre or post menopause.
_________________________
How often do women undergoing surgery for CPP or excision of endometriosis have an abnormal appendix (AE or other pathology)?
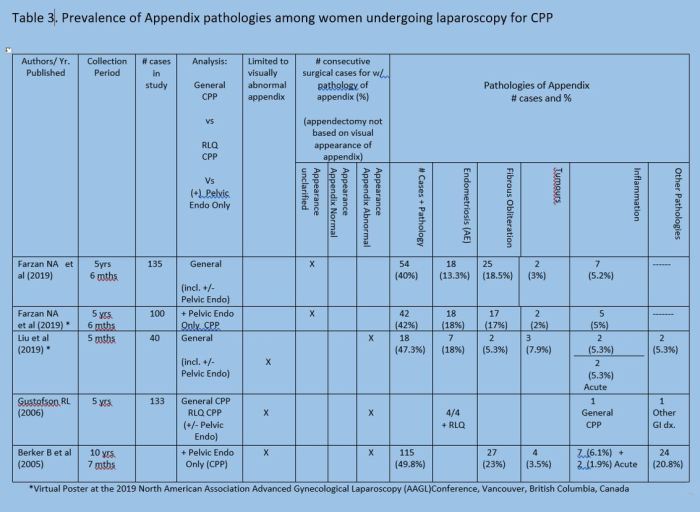
Citations Table 3 Prevalence of AE in Women Undergoing Surgery for CPP
- Persons with female reproductive organs and pelvic endometriosis have higher rates of AE and other abnormalities of the appendix than those with CPP and general population.(R)
- The presence of pathologies occurs among abnormal and normal (7,28) appearing Appendices (7,28)
“In cases of appendix involvement, intraoperative inspection may not show any alteration that suggests endometriosis. Then, the definitive diagnosis is confirmed through anatomopathological analysis”(28) – Denadi R et al. (2012)
- The presence of comorbid appendix pathologies is more frequent among those with pelvic endometriosis > those with CPP > general population.(30)
- Unclear if AE specific contributes to CPP however:
“In the case of the appendix, it could be proposed that the resultant adhesions and mass effect of the endometriosis could cause obstruction and lead to acute or intermittent appendicitis. Therefore, endometriosis of the appendix could complicate the already existent pelvic pain from the endometriosis not involving the appendix” (32)
– Berker B et al. (2005)
- The presence of AE was associated with dyspareunia among 54 women who underwent excision of endometriosis. (31)
“…appendiceal endometriosis is more related to the diagnosis of chronic pelvic pain usually associated with pelvic endometriosis” (28) – Denadi R et al. (2012)
Take it Or Leave It?
Traditionally seen as a remnant of our evolution without a purpose, new evidence suggests the appendix plays a role in replenishing ‘good bacteria’ after episodes of diarrhea. The occurrence of AE is increased among women with pelvic endometriosis and evidence suggests pathologies of the appendix as a comorbidity among these women is significantly higher in this population compared to women without endometriosis. Furthermore, presence of pathology is elevated even with a normal appearance. Based upon recent evidence, the removal of appendix at time of endometriosis excision is suggested by many surgeons.
“Some authors justify the prescription of appendectomy to patients with chronic abdominal pain with undefined origin, even when the organ (appendix) aspect is normal.” (28)
– Denadai R et al (2012)
Summary
- There are not a lot of data available, specific to AE. But suggestions around 1% of all persons with a endometriosis diagnosis and 3% of those with disease of the intestines.
- Prevalence of AE among specific populations: Pelvic Endometriosis > CPP > General Population.
- Prevalence of pathologies (any) of the appendix: Pelvic Endometriosis > CPP > General population.
- Recent comparative study of standard pathology slide protocol and modified protocol: modified slide protocol increased the number of confirmed dx of AE (significant).
- AE can occur alone or with pelvic endometriosis.
- AE occurs among adolescents through post menopause.
- AE is associated more with CPP than Acute Appendicitis or ‘Mimic’ condition.
- Women who develop Acute Appendicitis or ‘mimic’ presentation, more common without history of CPP and pain is localized to the RLQ. A small portion present with diffuse pain.
- Diffuse pelvic pain is more common among women with CPP and/or pelvic endometriosis that have comorbid AE or other pathology of the appendix. There may be tenderness at RLQ with palpation.
- Further, in women with CPP of unknown origin, the appendix, even if it appears normal, should be considered for removal due to increased probability that a pathological process may be present in the appendix.
- A high probability of comorbid pathology of the appendix among those with pelvic endometriosis > CPP lends to consideration of its removal at time of investigate laparoscopy for CPP or excision of endometriosis.
“Surgical texts present the gynecological aspects in detail (abt endometriosis), but the published literature on unexpected manifestations, such as appendiceal disease, is inadequate…the presentations to general surgeons may be atypical and pose diagnostic difficulty” (9) – Laskou S et al. (2011)
Web Page Appendiceal Endometriosis Citations
Extrapelvic Not Rare Endometriosis Education and Discussion Group
![]()
(last update 03/06/2021)

All Rights Reserved © 2020 Wendy Bingham, DPT Extrapelvic Not Rare